Identify the two major divisions of the nervous system.
Describe the common structures associated with these divisions.
Use the appropriate terms associated with signs of nervous system disorders.
Describe disorders of the nervous system, especially those associated with aging: Parkinson’s disease, myasthenia gravis, multiple sclerosis, and drug induced movement disorders, seizure disorders, stroke, tumors, inflammation and infections.
Identify related medications and treatments for disorders of the nervous system.
Discuss implications for nursing care and side effects of medications associated with major nervous system disorders.
Describe the actions and give examples of the following drug groups: CNS cerebral stimulants, respiratory stimulants, CNS depressants, narcotic and non-narcotic analgesics, antidepressants sedative/hypnotics, antipsychotics, anti-manic psychotherapeutic, and anti-parkinson's disease drugs.
Identify drugs that are often involved in drug abuse.
Describe general nursing care when giving medications for the nervous system.
List medications which may result in transient or permanent drug-induced movement disorders.
Describe several mental conditions for which psychotropic medications may be given as treatment.
List medications which may result in a high potential for the resident to fall.
Define pain.
Describe the advantage of scheduled pain medication versus PRN medication for chronic pain control.
Define placebo. Discuss the ethical issues associated with using placebos.
Nervous system-composed of the Central Nervous System (CNS)-brain and spinal cord; and the Peripheral Nervous System-connects the CNS to all parts of the body.
Refer to your textbook pg 423
Video on The nervous system: Click Here
Video on The Human Body:Nervous System: Click Here
More information on the Nervous System. Click Here
Major structures
Neurons-individual nerve cells-the primary functional unit.
Synapse-the junction between two neurons-a space between them, filled with transmission chemicals.
Nerves-bundles of neurons bound together by connective tissue.
Major functions-control bodily functions, conscious thought, sensory perceptions, motor functions, regulation of organs, blood vessels, other physical responses.
Brain is the control center for most of the vital bodily functions. Refer to your textbook pg 424-425
Spinal cord contains the motor and sensory pathways. Provides a pathway for impulses to and from the brain.
Autonomic nervous system (ANS)-means "self-controlling". Controls involuntary bodily functions such as glands, smooth muscle tissues of the blood vessels and GI tract, and heart. Includes sympathetic and parasympathetic systems.
Sympathetic- stimulating these nerve fibers usually produces vasoconstriction, rise in blood pressure, goose-flesh, pupils dilate, reduced saliva, slowing of activities, and acceleration of the heart rate.
Under conditions of stress, it prepares the body to meet an emergency.
Called the "flight or fight" system.
Parasympathetic - stimulating these nerve fibers usually produces vasodilation, fall in blood pressure, contraction of the pupil, increased saliva and GI activities, and slowing of the heart rate.
Restores and conserves body energy and brings the body back to normal conditions.
Disorders of the nervous system, especially associated with aging
Nervous system problems-general signs. Refer to your textbook pg 426
Pain-person senses discomfort, distress or suffering due to sensory nerve stimulation.
Tremor-trembling, quivering or involuntary movement.
Spasticity-an involuntary, abnormal increase in muscle tone or contraction.
Vertigo-dizziness, person has a sensation of moving around in space or objects moving around the person.
Dry mouth-lack of saliva or reduced saliva May be due to stimulation or over stimulation of the autonomic nervous system.
Loss of muscle control
Paralysis-inability to move.
Convulsions-involuntary muscular contraction and relaxation in an unsynchronized, irregular, contorted manner.
Coma-unconsciousness, deep stupor. Person cannot be aroused by external stimuli.
Stupor-being "in a daze”.
Insomnia-inability to sleep.
Aging-brings structural and functional changes. Refer to your textbook pg 426
Decrease in responses and reflexes.
Reduced muscle coordination.
Asthenia-weakness.
Decreased sensory reception.
Parkinson's Disease-slow progressive destruction of the nerve center in the brain responsible for body movement. Results in slow and decreased movement, muscular rigidity, resting tremor, and postural instability. Infrequent blinking, "mask-like" lack of facial expression. Fourth most common neurodegenerative disease of the elderly. Refer to your textbook pg 427
Side effects can be severe and require careful monitoring and documentation of behaviors, fluid intake, and temperature.
Safety is primary since either disease or medication can cause changes in motor responses. Resident may be mentally confused, unknowingly unsafe in ambulation.
Maintain adequate hydration.
Meals high in protein may interfere with drug absorption.
Physician's will often specify specific dosage times to ensure that plasma drug levels are constant during the daytime. If a specific time isordered, the drug must be administered within a 30 minute time frame. For example, drug is ordered for 10 AM. Drug must be administered between 9:30 AM and 10:30 AM.
May administer with a low protein snack if necessary.
Myasthenia Gravis-chemical deficiency at the synapse, causing episodic muscle fatigue, prolonged recovery in muscle activity. Lack of acetylcholine or excess of cholinesterase. May be caused by a significant immunological response. Refer to your textbook pg 427
Anti-myasthenics/anti-cholinesterase-block or reduce available cholinesterase.
Neostigmine (prostigmin)
Pyrldostigmine (Mestinon, Regonol)
Nursing care and side effects:
Diarrhea and abdominal cramps.
Increased sweating and salivation.
Nausea and vomiting.
Difficult defecation and urination.
Other medications may be combined to relieve side effects.
Careful monitoring of drug therapies and observation of effects.
Corticosteroids-Reduce the body’s immune response, reducing inflammation.
Prednisone (Deltasone)
Nursing care and side effects:
Stomach upset, diarrhea.
Increased appetite.
Fluid retention.
Agitation.
May need to restrict sodium to control fluid retention.
Give with food to reduce gastrointestinal (01) upset.
Very potent medication with numerous side effects and drug interactions; monitor resident's response.
Immunosuppressants-reduces the natural immune response.
Azathioprine (Imuran)
Nursing care and side effects:
Increased risk for cancer
Nausea and vomiting
Changes in blood count especially white blood count (WBCs)
Increased risk for infections, infectious diseases (communicable diseases)
Skin rash
Bleeding or bruising
Giving the medication after meals or at bedtime may lessen GI upset.
Multiple Sclerosis (MS)-the outer covering of the nerves (myelin sheath) is destroyed, disrupting impulse conduction. May be intermittent with lengthy remissions. Symptoms include blurred vision, paralysis, speech problems, numbness, unsteady gait; progressive. Refer to your textbook pg 427
Seizure disorders-Seizures may range from staring spells to prolonged convulsive movements. Residents may exhibit one or more of the following:
Video on a gentleman in the hospital having a seizure. If you have never witnessed a person having a seizure this is a clip to watch; Click Here
Impaired consciousness
Excess or loss of muscle tone or movement
Disturbed behavior and/or mood
Involuntary urination and defecation
Refer to your textbook pg 428
Related medications and treatment:
Anticonvulsants-block nerve impulses that cause seizures.
Phenytoin sodium (Dilantin)
Primidone (Mysoline)
Divalproex sodium(Depakote)
Carbamazepine (Tegretol)
Barbiturates, Phenobarbital (Nembutal)
Benzodiazepines (Klonopin, Valium)
Nursing care and side effects:
Minimize alcohol use.
Normal activities should be encouraged.
During a seizure, protect resident from injury. Do not attempt to 'protect' tongue as the resident or you could be injured. Loosen clothing, especially around the neck, place head on pillow. If possible, roll onto side to prevent aspiration of secretions or vomitus.
Usually drug treatment includes more than one type of medication. Be aware of toxic effects or cumulative effects.
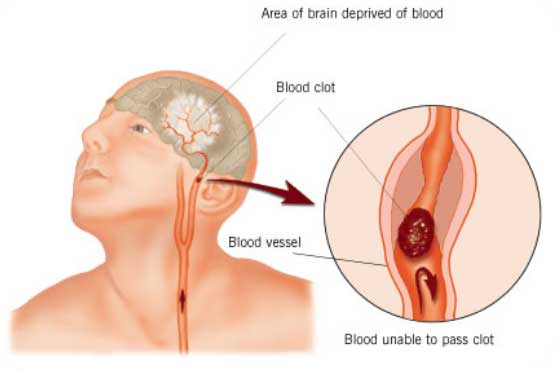
Stroke-interruption of the blood supply to the brain with tissue death in a portion of the brain. Refer to your textbook pg 42-429
Thrombosis-blood clot in a blood vessel in the brain or neck.
Cerebral embolism-fat globules, air, or blood clot from heart occludes circulation to a portion of the brain.
Ischemia-decreased blood flow to an area of the brain.
Cerebral hemorrhage-rupture of a cerebral blood vessel with bleeding into brain tissue causing pressure and death of tissue.
A stroke can occur without warning. Symptoms may include one or more of the following:
Dizziness (vertigo)
Memory loss
Headache
Fainting
Blurred vision
Speech difficulty
Loss of balance
Partial paralysis
Related medication and treatment:
Anticoagulants or drugs to prevent clot formation may be used depending on the type and extent of injury.
Heparin (administered subcutaneously or intravenous by licensed nurse)
Warfarin (Coumadin)
Nursing care and side effects:
Bleeding, bruising.
Monitor for signs of excessive bleeding from minor injuries. Report bleeding gums, unusual bruising, black tarry stools and blood in the urine.
Prothrombin times (PT) or INR (International normalized ratio) will be conducted by a laboratory frequently until the correct dose is established. Laboratory tests will be conducted at least every three to four weeks as long as the resident is on an anticoagulant. Results of tests must be communicated to the resident's physician by the licensed nurse promptly. Physician will adjust the dose of blood thinning medication based on the results of the laboratory tests.
Resident should avoid alcohol, salicylates (aspirin, numerous products over the counter which have ASA as base ingredient).
May cause orange color if urine is alkaline.
Tumors-abnormal growth in the brain. A tumor may originate in the brain or metastasize or migrate from another site in the body. Refer to your textbook pg 431
Infection and inflammation Refer to your textbook pg 431
Encephalitis is an inflammation of the brain.
Meningitis is an inflammation of the lining of the brain and spinal cord.
Treatment depends upon the causative organism. Some infections can only be treated symptomatically.
Antibiotics and non-steroidal anti-inflammatory drugs, immunosuppressants and anticonvulsants may be used. The blood brain barrier prevents many medications from reaching the areas of the brain affected by an infection.
Other categories of medications used in treating nervous system disorders.
CNS Stimulants-there are three general categories of CNS stimulants: cerebral stimulants, respiratory stimulants and antidepressants. These drugs are often abused due to the effect of euphoria, a false sense of well-being. Cerebral stimulants-"speed" up brain activity and other body functions. Clinical use is limited but may be used in depression, obesity, hyperactivity in ADD children, narcolepsy. Refer to your textbook pg 431
Examples of CNS stimulants
Methylphenidate (Ritalin)
Pemoline (Cylert)
Caffeine (Vivarin, No Doz)
Amphetamine (Dexedrine, Desoxyu)
Nursing care and side effects:
Causes excitement, dizziness, dry mouth.
Restlessness.
Palpitation (irregular heart rhythm).
Give early in the day so the stimulating action does not interfere with sleep.
CNS depressants-depress or slow the functions of the CNS. Include sedatives, analgesics, tranquilizers, anticonvulsants. Refer to your textbook pg 432-433
Oral Opioid analgesics for moderate to severe pain.
Codeine
Oxycodone
Morphine sulfate (MS)
Hydromorphone (Dilaudid)
Dosing interval for the above drugs is every 4 hours or less.
Analgesics-pain medications. Antipyretic analgesics (acetaminophen, aspirin, ibuprofen, naproxen) also reduce fever. Refer to your textbook pg 432
NOTE Total daily dosage of acetaminophen should not exceed 4 Gm in 24 hours.
Non-Opioid Analgesic Medications for Mild or Moderate Pain
Acetaminophen (Tylenol)
Aspirin (ASA)
Ibuprofen (Motrin, Nuprin)
Naproxen (Aleve)
Buffered aspirin (Ascriptin, Bufferin)
Nabumetone (Relafen)
Salsalate (Mono-Gesic, Disalcid)
Tolmetin (Tolectin)
Note: Acetaminophen is non-effective on inflammation.
Common side effects of pain medications
Constipation.
Drowsiness.
Dizziness.
Respiratory depression.
May cause paradoxical excitement in the elderly.
Aspirin (ASA}-Give with food to reduce gastric upset. Can interfere with blood clotting. Residents receiving Coumadin must not take aspirin or any medications containing aspirin.
Acetaminophen (Tylenol)-liver damage.
Ibuprofen (Motrin)-kidney failure, OJ bleeding.
Pain management in the elderly Refer to your textbook pg 435
Almost all medications which relieve pain, cause constipation. The supervising licensed nurse should ensure that there is an order to treat constipation. Report to nurse if resident does not respond to treatment for constipation.
Believe the resident's report of pain.
World Health Organization three step-analgesic ladder is the standard of practice for pain control
Mild pain--ASA, Tylenol, non steroidal anti-inflammatory drugs (NSAIDS)
Moderate Pain-weak opioids with or without non-opioids Tylenol #3
Severe Pain-potent opioids, morphine with or without non-opioids
Schedule doses on a regular basis (i.e., "by the clock") to maintain the level of drug that will help prevent recurrence of pain. Physician may order additional doses or medications for "breakthrough" pain.
Ask and record resident's report of level of pain. Most facilities use a 10 point pain scale.
Report to supervising licensed nurse when resident reports that pain is not relieved by ordered medication(s).
Use non-drug measures to promote comfort.
Anxiety increases perception and intensity of pain.
Residents with cognitive deficits may not be able to verbalize the need for pain relief. Observe behavior. Increased restlessness or irritability may be due to pain.
Report to supervising nurse when a resident expresses fear of addiction or that pain medication must be "saved" until pain is severe.
Definitions related to issues of addiction established by the American Pain
Society:
Psychologic dependence. A pattern of compulsive drug use characterized by continued craving for an opioid and the need to use the opioid for effects other than pain relief or for non medical reasons.
Physical dependence. The occurrence of withdrawal symptoms when an opioid is suddenly stopped or an opioid antagonist is administered. Withdrawal symptoms usually can be controlled by gradually withdrawing the drug.
Tolerance. The resident experiences a decrease in the analgesic effect of the drug. Tolerance to analgesia may be treated with increased doses of the drug. However, in most instances, disease progression, not tolerance to the drug is the primary reason for increasing drug dosage.
Addiction. An acquired, chronic disease characterized by a persistent pattern of dysfunctional drug use (for non medical reasons) and aberrant (abnormal) behavior involving loss of control over use and continued use despite diverse physiologic, psychologic, and/or social consequences. A pattern of compulsive drug use characterized by a continued craving for the opioid and the need to use the opioid for effects other than pain relief. Fewer than 1%ofpatients develop addiction to a medically prescribed opioid.
Psychotropic drugs-given to treat mental conditions such as anxiety, depression, and psychosis. Also known as psychoactive or psychotherapeutic drugs.
Antidepressants-several different classes with different modes of action. The newer SSRl (selective serotonin reuptake inhibitors) are generally preferred for use in elderly because of a relatively low incidence of harmful effects. Some have a sedating affect while others result in a more stimulating therapeutic effect
Monoamine Oxidase Inhibitors (MAOI)
Phenelzine (Nardil)
Tranylcypromine (pamate)
Tricyclic Antidepressants (TCA)-* indicates that the drug is not recommended for use in the elderly.
Note: Elavil and Limbitrol may be the drug of choice for treating neurogenic pain (such as trigeminal neuralgia, peripheral neuropathy).
Selective Serotonin Reuptake Inhibitors (SSRI)
Fluoxetine (prozac)
Paroxetine (Paxil)
Sertraline (Zoloft)
Other: Bupropion (Wellbutrin)-may cause seizures, therefore is usually not the drug of first choice.
Nursing care and side effects:
For MAOIs
Therapeutic effect maybe noted in one week or may take up to three to four weeks.
Postural hypotension can place resident at risk for falls.
Can cause dangerous reactions with other psychotherapeutic medications.
Monitor for constipation.
Must avoid pickled fish or meats, dairy products (cheese, yogurt), alcohol, non-alcohol beer or wine, yeast extracts and coffee.
Usually selected when other types of therapy have failed.
For TCAs
Sedating effect. Administer at bedtime.
Administer just before or after meal to reduce GI irritation.
Monitor for blood pressure and pulse rate in residents with preexisting cardiovascular disease. Report a rise or fall in the systolic pressure or sudden change in pulse rate to supervising nurse.
Some of these drugs have a prolonged half-life which means it may be days or weeks before the entire drug has been metabolized and excreted from the body.
Should never be given with MAOIs due to serious, sometimes fatal interactions.
Can be either stimulating or sedating, depending on product. Monitor for restlessness and anxiety.
May increase or decrease appetite.
Nausea, diarrhea/loose stools, dyspepsia
Tremor
Sexual dysfunction
Dry mouth
Tranquilizers-act as depressants to the central nervous system and are used to calm, induce sleep, or decrease anxiety.
Sedative/hypnotic drugs ("minor tranquilizers, the more common tranquilizers") must be used with caution in the elderly.
Barbiturates cause adverse effects in the elderly. Use is generally limited to controlling seizures. Can depress respirations, cause paradoxical excitation in elderly and "hang-over" effect. • Phenobarbital
Hypnotics produce sleep but interfere with normal sleep cycles. Should only be used for short-term.
Flurazepam (Dalmane)
Ethchlorvynol (Placidyl)
Temazepam (Restoril)
Hypnotics should be used for no longer than two weeks. Non-drug methods to assist the resident to sleep should be initiated.
Antihistamines can induce drowsiness and sleep, but have anti-cholinergic effects causing constipation, dry mouth, orthostatic hypotension, difficulty voiding and confusion in elderly. The use of Benadryl and other antihistamines for sleep is strongly discouraged in the literature.
Long-Acting Benzodiazepines - Management of anxiety disorders and for short term relief of anxiety symptoms.
Diazepam (Valium)
Drug of choice for status epilepticus.
Long half life. Therefore can have cumulative effect in elders.
Chlordiazepoxide (Librium)
Clorazepate (Tranxene)
Clonazepam (Klonopin)
Quazepam (Doral)
Halazepam (Paxipam)
Nursing care and side effects:
Side effects of the above drugs include drowsiness, ataxia, confusion, constipation, urinary retention and hypotension.
Avoid the use of caffeine and alcohol.
Habituation may occur. Dose reduction must be performed gradually overtime.
Not recommended for use in elders.
Short-Acting Benzodiazepines - Management of anxiety disorders and for short term relief of symptoms of anxiety.
Alprazolam (Xanax)
Lorazepam (Ativan)
Oxazepam (Serax)
Nursing care and side effects:
The half life of the above drugs is less than 24 hours. Therefore, there is less cumulative effect.
Side effects include drowsiness and sedation which usually disappear with continued use or a reduced dosage.
May experience hypotension, and blurred vision.
Avoid the use of caffeine and alcohol.
Hydroxyzine HCL-anti-pruritic (relieves itching), antihistamine, antiemetic and used to treat anxiety, tension, and psychomotor agitation.
Atarax, Vistaril
Nursing care and side effects:
Watch resident for drowsiness.
Dry mouth is a significant problem. Avoid abrasion of the gums.
Provide good oral care.
Neuroleptics (referred to as "major tranquilizers")-most commonly prescribed as antipsychotics; used to treat psychotic disorders and manage non psychotic behavior symptoms of persons with dementia.
Thioridazine HCL (Mellaril)
Chlorpromazine (Thorazine)
Haloperidol (Haldol)
Nursing care and side effects:
Constipation
Drowsiness
Dizziness
Blurred vision
Orthostatic hypotension
"Extrapramidal symptoms"-restlessness, muscle spasms, symptoms like Parkinson's disease.
Must not be combined with alcohol-potentiates sedation of tranquilizer.
High doses of major tranquilizers may cause tardive dyskinesia.
Symptoms include abnormal movements of the extremities, in and out movement of tongue, sucking and smacking lips, lateral jaw movements.
Reduced awareness of thirst.
Abrupt withdrawal may cause seizures.
Monitor for postural hypotension by taking blood pressure just before each dose of the drug with the resident standing, and check with supervising licensed nurse if systolic pressure is less than 90.
Anti-manic psychotherapeutic-control and prevent manic (hyper-activity) episodes due to bipolar disorders.
Unusual fluid or salt loss from body may result in toxicity. Observe for and report profuse sweating, diarrhea or vomiting.
Toxicity symptoms include nausea, tremor, muscle weakness.
Placebos-a tablet containing presumably inert ingredients rather than active drug ingredient-also are called "sugar" pills, though placebos aren't strictly composed of sugar. Placebos mayor may not be effective. There is some search that suggests that they enhance the effects of the body's own biochemical’s called endorphins. Endorphins work to reduce pain and produce a sense of well-being. Placebos are used only in certain circumstances, such as for research, and must only be given with the resident's knowledge and approval.
Drug-induced Movement Disorders-this is the result of widespread use of phenothiazine, thioxanthene, and butyrophenone antipsychotic and antiemetic medications. All of these drugs block CNS dopamine receptors, which may result in drug-related syndromes mimicking spontaneously occurring neurological disorders. Extrapyramidal (involuntary movements or jerking of limbs or facial muscles) effects of newer antipsychotic may still occur.
Caution should always be exercised in the administration of these drugs.
 Unit 14
Unit 14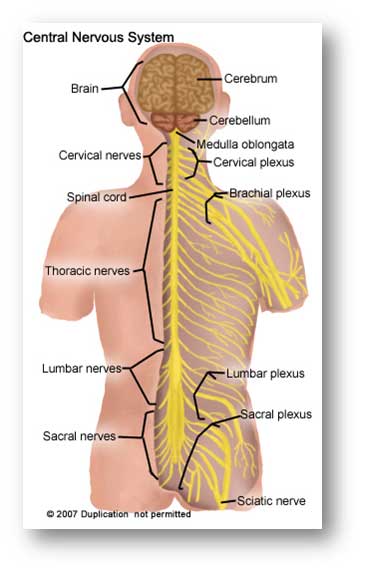 Refer to your textbook Ch 17
Refer to your textbook Ch 17 
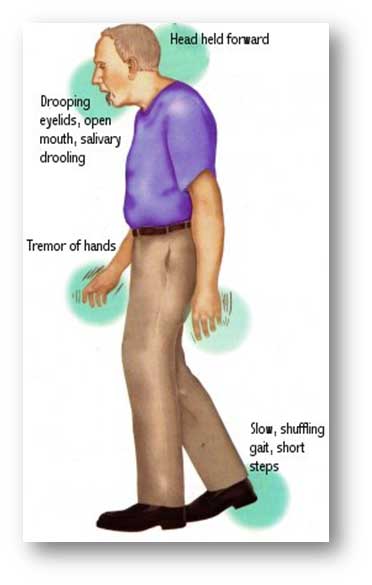 Parkinson's Disease-slow progressive destruction of the nerve center in the brain responsible for body movement. Results in slow and decreased movement, muscular rigidity, resting tremor, and postural instability. Infrequent blinking, "mask-like" lack of facial expression. Fourth most common neurodegenerative disease of the elderly. Refer to your textbook pg 427
Parkinson's Disease-slow progressive destruction of the nerve center in the brain responsible for body movement. Results in slow and decreased movement, muscular rigidity, resting tremor, and postural instability. Infrequent blinking, "mask-like" lack of facial expression. Fourth most common neurodegenerative disease of the elderly. Refer to your textbook pg 427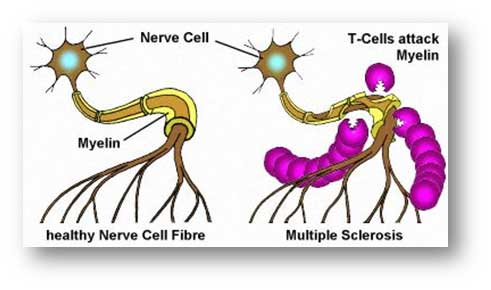
 Stroke-interruption of the blood supply to the brain with tissue death in a portion of the brain. Refer to your textbook pg 42-429
Stroke-interruption of the blood supply to the brain with tissue death in a portion of the brain. Refer to your textbook pg 42-429

 Antihistamines can induce drowsiness and sleep, but have anti-cholinergic effects causing constipation, dry mouth, orthostatic hypotension, difficulty voiding and confusion in elderly. The use of Benadryl and other antihistamines for sleep is strongly discouraged in the literature.
Antihistamines can induce drowsiness and sleep, but have anti-cholinergic effects causing constipation, dry mouth, orthostatic hypotension, difficulty voiding and confusion in elderly. The use of Benadryl and other antihistamines for sleep is strongly discouraged in the literature. at suggests that they enhance the effects of the body's own biochemical’s called endorphins. Endorphins work to reduce pain and produce a sense of well-being. Placebos are used only in certain circumstances, such as for research, and must only be given with the resident's knowledge and approval.
at suggests that they enhance the effects of the body's own biochemical’s called endorphins. Endorphins work to reduce pain and produce a sense of well-being. Placebos are used only in certain circumstances, such as for research, and must only be given with the resident's knowledge and approval.